Crimean-Congo haemorrhagic fever virus
Issue: Arboviruses and their Vectors
06 August 2019 article
Crimean-Congo haemorrhagic fever virus (CCHFV) is a neglected virus identified as a key research target by the World Health Organization (WHO). Following the unpredicted size, speed and reach of the Ebola virus outbreak in West Africa in 2014, the WHO assembled a broad coalition of international experts to develop a research and development (R&D) Blueprint for action to prevent future disease epidemics caused by under-researched pathogens. This Blueprint highlights the importance of increased research investment into CCHFV by researchers, pharmaceutical communities and governments.
CCHF is a rare tick-borne disease spread to humans from animals and causes high human fatality rates. It is caused by a negative-sense single-stranded, segmented RNA virus classified within the Orthonairovirus genus of the family Nairoviridae. The virus is particularly associated with Hyalomma ticks, which act as both reservoirs and vectors. Because of this association, it is the most widely distributed agent of severe haemorrhagic fever known, endemic over much of Asia, and with focal endemic areas over Africa and Europe where it continues to emerge.
History and politics
Classical evidence points to a probable description of CCHF in the territory now occupied by Tajikistan as early as 1100 AD, in reports of patients with bleeding symptoms that were linked to blood-sucking ticks. The first modern medical account of disease was made much later in 1944 during an outbreak affecting over 200 Soviet troops assisting in war-devastated Crimea. This disease was named Crimean haemorrhagic fever (CHF) and was shown to be distributed across the Soviet Republics. While it was established that a virus was the cause of this disease, it was not isolated and sent for registration by the Soviet scientists until 1968. During the registration process, CHF virus was recognised as identical to an African virus – Congo virus – that had been isolated in 1956 and registered in 1961 by virologists from the Congo, USA and UK. It came as a great surprise to Soviet virologists that a virus causing an African disease, that did not even have a name before 1961, could be associated with CHF which had been recognised and studied for nearly three decades in the USSR. Surprise turned to shock when, by convention, it was advised that the official name should be Congo virus, since this virus had been described and registered in the catalogue of arthropod-borne viruses before CHF virus. Shock among the Soviet virologists turned to outrage since they had used a different name for the disease for many years and they refused to use the new nomenclature. This was the time of the Cold War and although the International Committee for Taxonomy of Viruses suggested the compromise name of Congo-Crimean haemorrhagic fever virus, the deadlock was not resolved until 1973 when the Soviet compromise ‘Crimean-Congo haemorrhagic fever virus’ was finally agreed.
Human disease and basic biology
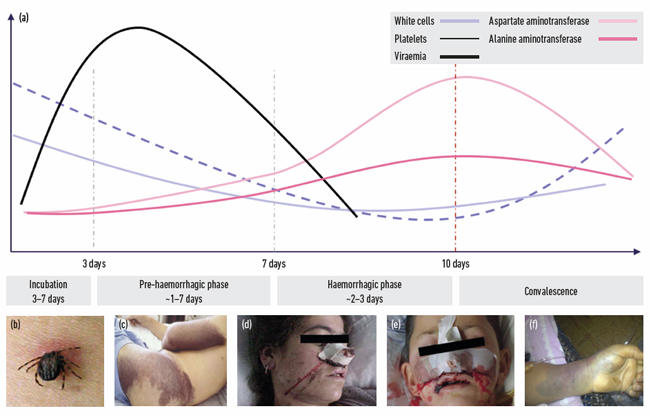
CCHFV infects a wide range of domestic and wild animals, such as cattle, goats, sheep, hares and rodents, which all serve as asymptomatic amplifying hosts for the virus. Humans are incidental hosts which often acquire the virus through tick bites. Unlike many other tick-borne viruses, CCHFV is also transmitted by direct contact with infected tissues and body fluids of animals and humans. Human-to-human transmission is a common hallmark of infection which can lead to population-based and nosocomial outbreaks. Clinical features commonly include an abrupt onset of fever, myalgia, headache and thrombocytopenia which can progress to haemorrhage, multiorgan failure and death (Fig. 1). Case fatality rates (CFRs) correlate with the mode of transmission: tick bites lead to CFRs of 10–30 % but incidents of up to 80 % are often reported following nosocomial transmission. Human transmission resulting from the butchering of viraemic animals is also common and can lead to high mortality. Increased episodes and small outbreaks have been noted to coincide with religious festivals that involve the slaughter of (viraemic) animals. This is expected to play an important role in increased transmission in the future, as the dates of such festivals overlap with increased tick feeding activity and viraemic animals.
CCHF is nevertheless a rare disease, with approximately 2,000 cases per year globally. Early diagnosis is important for the implementation of adequate infection control and contributes to a favourable outcome through the general supportive management of symptoms. Administration of the antiviral ribavirin is thought to be effective if used early in infection, but this is based on observational studies; a large placebo-controlled, randomised control trial is lacking, and evidence of the efficacy of ribavirin for the treatment of CCHF infections remains inconclusive. Likewise, there are no effective vaccines licenced for use against CCHF. In consequence, the Advisory Committee on Dangerous Pathogens in the UK classifies the virus as a hazard group 4 pathogen, which mandates that all work with infectious materials be carried out at maximum biological containment in specialist containment level 4 (CL4) facilities. Corresponding classifications apply in other parts of the world and generally the availability of such resource-heavy laboratory infrastructure is a bottleneck to basic research. Consequently, knowledge of CCHFV has lagged behind that of other pathogens and the poor payback on investment required for applied research into therapeutics and vaccine development for such a rare disease has been a major impediment to progress.
Nevertheless, some aspects of CCHFV’s biology are known or can be inferred from work on similar orthonairoviruses. Its genome consists of three single-stranded, negative-sense RNA molecules, termed S (small), M (medium) and L (large), encoding the N-protein (S-segment), the viral glycoprotein (M-segment) and the viral RNA-dependent RNA polymerase (RdRp) (L-segment). Infection starts with viral attachment to an unknown cell-surface receptor and entry via endosomes. Viral fusion with the host cell membrane is thought to be pH-dependent, releasing the viral ribonuclear-protein-complex into the cytoplasm. L- and S-segment mRNAs are translated by free ribosomes while M-segment mRNA is translated by membrane-bound ribosomes and is co-translationally cleaved to yield two glycoproteins, Gn and Gc. These accumulate in the Golgi, where virions assemble and bud, being released after fusion with the plasma membrane.
|
|
Fig. 1. (a) The general clinical features of CCHF infection can be defined into four distinct phases: incubation, a pre-haemorrhagic phase typified by fever, myalgia, nausea; a haemorrhagic phase typified by bruising, epistaxis and haematemesis; followed by convalescence. Patients do not always develop haemorrhagic symptoms. Some infections |
Molecular epidemiology diagnostics and vaccine interventions
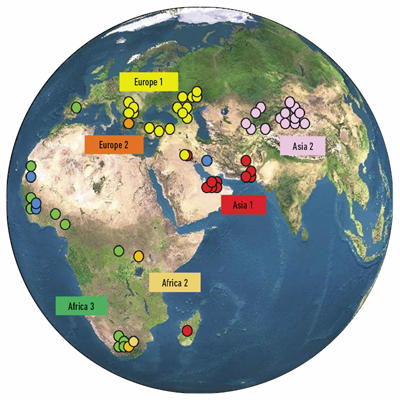
While serological methods have been important in determining the breadth of CCHF distribution, these approaches do not readily differentiate between alternative strains of CCHFV. To characterise viral strains in more detail and facilitate a global epidemiological study, molecular methods based on partial and complete sequence data of the S-segment have been used to identify certain S-segment genotypes. These genotypes show a strong relationship to the geographical area of isolation of the parent virus, leading to the terminology Asia 1, Asia 2, Europe 1, etc. These studies also show that similar genotypes are found in distant geographical locations (Fig. 2), supporting the idea that the virus or infected ticks may be carried over long distances during bird migration. Anthropogenic factors, such as the trade in livestock, also appear to play a role in the dispersal of CCHF viruses.
|
|
Geographical correlation of genotypes. When superimposed onto the globe the phylogenetic grouping of S RNA segments illustrates that the pattern of genetic diversity observed is largely related to the geographical distribution of the viruses. Similar genotypes are sometimes found in distant geographical locations, highlighting long-distance carriage of virus in infected ticks during bird migration and or trade in livestock. The recent emergence of CCHF in Spain is thought to be the result of bird migration from West Africa. |
With the increasing applicability of whole genome sequencing to the many different strains of virus it has become clear that CCHFV shows enormous variety. While simple genetic drift and recombination play important roles, segment reassortment seems to be a key driver of genetic variation, with current evidence pointing to the greater exchange of M-segments between viruses. Co-infections of multiple CCHFV strains are a prerequisite of such variation and most likely the optimal environments occur within ticks, where lasting virus infections persist for extended periods, and superinfection with a second or third strain during blood meals may be quite common. These observations provide support for a global and dynamic reservoir of CCHFV and underpin the importance of maintaining diagnostics that keep pace with such variation. This is important so that all known circulating strains can be promptly identified and, in the case of human infection, rapidly controlled before infection spreads.
While vaccine interventions for CCHFV are currently unavailable, this research area is now highly active, and several approaches are being developed. One of the most advanced is a viral-vector approach based on the highly successful Modified Vaccinia Ankara approach which drives the expression of CCHFV-GP. Phase I clinical trials should commence early in 2020.

Roger Hewson
Roger Hewson is Scientific Leader for Viral Haemorrhagic Fevers and Arboviruses at Public Health England – Porton Down and Head of the institute’s WHO Collaborating Centre for Virus Research and Reference.
What does a typical day or week look like for you?
The Virology & Pathogenesis Laboratory studies a wide range of zoonotic and vector-borne viruses, many of which are new and emerging, including to the UK. A typical week involves lab meetings and one-to-one discussions on current research projects, the preparation and finishing touches to scientific reports for publication, including the supervision of MSc and PhD students. International collaborations and laboratory networks, including with partners in endemic disease regions, is an important aspect of our work and we need to be involved in workshops and occasionally field work to support our basic capability – travel or planning for such activity is a central theme of the laboratory. Advancing our research through new proposals and grant applications for new sources of funding to sustain capacity is a constant necessity.
What advice would you give to someone starting out in the field?
Follow your interests, develop trustworthy experimental capability, develop a niche and keep pace with technological advances.
Images: Coloured scanning electron micrograph of CCHF viral particles (yellow) budding from the surface of cultured epithelial cells from a patient. National Institute of Allergy and Infectious Diseases, NIH/Science Photo Library.
Fig. 1. Graph modified from Ergonul 2006. Pictures from collaborators: Prof. Salih Ahmeti, Kosovo & Farida Tishkova, Tajikistan.
Fig. 2. Roger Hewson.