Dengue and the introduction of mosquito-transmitted viruses into Australia
Issue: The Mobile Microbe
08 November 2016 article
Dengue virus outbreaks involving 100s of cases periodically occur in north Queensland, the area of Australia where the primary mosquito vector, Aedes aegypti, occurs. This article summarises the ecology, history, current situation and control of dengue virus transmission in Australia and examines the threat posed by newly emergent arboviruses, such as Zika and chikungunya viruses.
Dengue viruses
Each year, across tropical and sub-tropical regions of the world, an estimated 390 million people are infected with one of the four serotypes of dengue virus (DENV). The DENVs are single-strand positive sense RNA viruses of the genus Flavivirus, which also includes mosquito-borne viruses such as yellow fever (YFV), Zika (ZIKV), Japanese encephalitis (JEV) and West Nile (WNV) viruses. About a quarter of infections with DENV are symptomatic. So called ‘classic dengue fever’ is characterised by fever, rash, headache, and muscle and joint pain. Severe and potentially fatal disease occurs in about 1% of cases of DENV infection. This is characterised by plasma leakage with or without haemorrhage.
The DENVs are predominately transmitted between humans by the mosquito, Aedes aegypti, which has adapted its lifestyle to human habitation. Biological traits of this species that enhance its ability to serve as a vector of DENVs are: (1) it feeds almost exclusively on humans; (2) multiple blood feeding behaviour whereby a single female can bite several times to obtain a blood meal, thus potentially infecting numerous people; (3) adaptation to use man-made containers, such as tyres and potplant bases, as larval habitats; and (4) it prefers to feed and rest indoors.
The Asian tiger mosquito, Aedes albopictus, can also efficiently transmit DENVs and has driven outbreaks in locations where Ae. aegypti is absent or are in low numbers. However, Ae. albopictus does not share the same anthropophilic ecology as Ae. aegypti and so outbreaks caused by this species are generally not of the same magnitude as those driven by Ae. aegypti.
Dengue in Australia
The DENVs are not endemic to Australia, but are intermittently introduced by infected travellers. Disease attributed to DENV infection has occurred historically in Australia since the 1800s. Early outbreaks involved 1000s of cases and whilst primarily focussed in northern Queensland, transmission extended as far south as Gosford in New South Wales. For instance, the 1904–05 epidemic in Brisbane infected 75% of the population and was associated with 94 deaths. One of the largest and most widespread epidemics occurred in 1954–55 and it was estimated that at least 15 000 people were affected in Townsville alone. Following this epidemic, out- breaks of dengue ceased in Australia for 26 years, coinciding with a contraction in the geographical range of Ae. aegypti. This contraction was due to a decline in rainwater tank usage via reticulation of water supplies, improved sanitation, use of residual insecticides by homeowners, and the invention of the motor mower and the resulting improvement in the maintenance of domestic backyards.
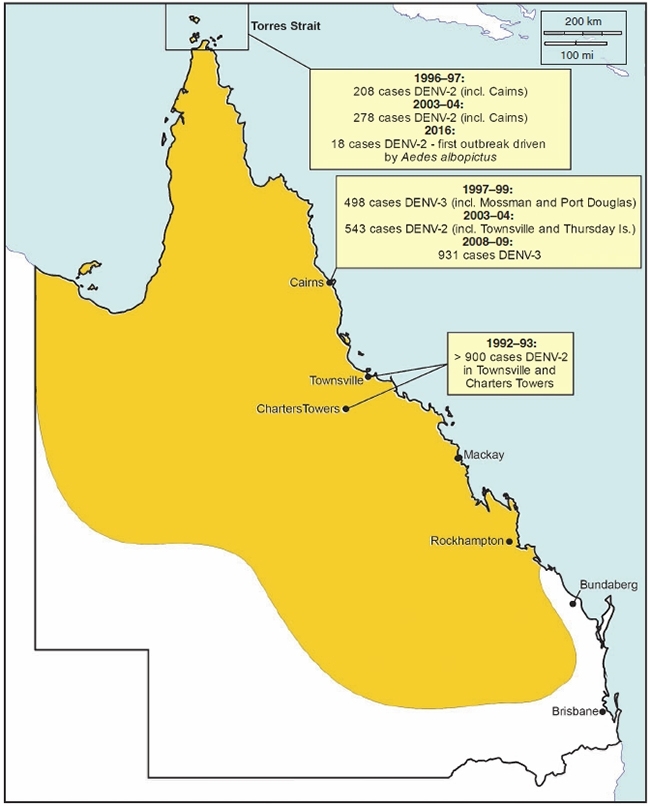
DENV reappeared in 1981, causing an outbreak across multiple localities in north Queensland. The frequency of dengue outbreaks has increased dramatically in the last 25 years. This increase can be attributed to a number of factors, including (1) epidemic DENV transmission in neighbouring countries; (2) increased arrivals from dengue active countries into international airports in Cairns and Townsville, which were opened in the mid-1980s; and (3) high populations of Ae. aegypti. Tourists taking advantage of low cost flights to Bali, fly-in, fly-out workers to Papua New Guinea and family visits have accounted for a considerable proportion of imports into Cairns in recent years. Although there have been almost 50 outbreaks in this time, they are usually of short duration and involve less than 100 cases. Larger outbreaks sporadically occur, involving 100s of cases, often across multiple locations and over several months (Figure 1). The largest outbreak in 50 years occurred in Cairns in 2008–09 when almost 1000 cases of DENV-3 were reported. The explosiveness of this outbreak was attributed to unseasonably hot weather and above average rainfall leading into the wet season, coupled with delays in case notification and a shortened extrinsic incubation period of the DENV-3 strain in Ae. aegypti.
FIGURE 1. MAP OF QUEENSLAND SHOWING THE CURRENT RANGE OF AEDES AEGYPTI (SHADED GOLD) AND SIGNIFICANT DENGUE OUTBREAKS SINCE 1992. THE LOCATIONS IN PARENTHESES ALSO REPORTED CASES THAT WERE LINKED TO THE PRIMARY EPICENTRE OF THE OUTBREAK. THE DISTRIBUTION OF AEDES ALBOPICTUS IS RESTRICTED TO THE TORRES STRAIT.
Dengue control in Australia
In the absence of an effective DENV vaccine or specific antiviral treatment, the primary disease control strategy is suppression of Ae. aegypti and/or Ae. albopictus populations. This involves elimination of containers in which larvae develop by removing them or treating them with methoprene, an insect growth regulator which interferes with mosquito metamorphosis. Adult control is also implemented during episodes of local transmission and involves targeted spraying of indoor resting places of Ae. aegypti with residual pyrethroid insecticides. Considerable success has been achieved in the control of Ae. albopictus is the Torres Strait when harbourage spraying of resting sites with pyrethroids has been used to supplement larval control. The success of interventions to limit local transmission is dependent on timely notification of suspected cases. Delays in case notification can result in a second generation of cases before control measures are initiated, which contributes to the rapid acceleration of some dengue outbreaks.
Although they are effective, chemical-based control methods are relatively expensive, labour-intensive and there is the potential for mosquitoes to develop resistance to the insecticide being applied. A promising control strategy that had its first field evaluations in north Queensland in 2011 is the release of Ae. aegypti trans-infected with the endosymbiotic bacterium Wolbachia. Wolbachia reduces the ability of the mosquito to transmit DENVs. Field releases in the Cairns region and Townsville have been very successful, reaching almost 100% fixation of Wolbachia within the Ae. aegypti population. Encouragingly, strong DENV blocking within the mosquito continues at least one year post release. Because this technology is still in its infancy, it is too early to determine the effect of Wolbachia releases on the frequency and magnitude of DENV transmission amongst the human population in north Queensland.
The global march of other Aedes-transmitted viruses
Although local transmission of DENVs occurs all too regularly, Australia has so far been spared from the spectre of chikungunya virus (CHIKV) and ZIKV, which are also transmitted by Ae. aegypti and Ae. albopictus. CHIKV causes crippling arthralgia and has undergone a global expansion since 2004 that has afflicted millions of people on multiple continents. ZIKV has gone from causing an obscure non-specific febrile illness to being associated with neuro- logical disease syndromes including Guillain-Barré syndrome (a form of paralysis) and congenital birth defects, most notably microcephaly, during its march through the western Pacific and South America. Despite over 550 and 66 imported cases of CHIKV and ZIKV, respectively, being notified in Australia as of August 2016, local transmission has not been reported. This is likely because most cases have been reported outside of areas where Ae. aegypti and Ae. albopictus exist and comprehensive control actions have been rapidly undertaken in response to notified cases in north Queensland.
Restricted to Africa and South America, YFV causes episodic outbreaks of acute haemorrhagic disease which have the potential to spread to other areas of the world, as evidenced by 11 imported cases into China from an outbreak in Angola that began in December 2015. However, the risk of a YFV epidemic occurring in Australia is expected to be low, as travellers from endemic areas must be vaccinated against the virus.
The future
Due to the presence of Ae. aegypti and infected travellers, the DENVs will continue to be a threat to north Queensland. Current control programmes have undoubtedly limited the severity of DENV outbreaks and the Wolbachia-based approach may provide an alternative to the use of insecticides in the future.
Any geographical expansion of Ae. aegypti or the establishment of Ae. albopictus in temperate regions could render populated cities of eastern Australia, such as Brisbane and Sydney, receptive to outbreaks of DENVs, CHIKV or ZIKV. Comprehensive surveillance to detect the presence of these two species and rapid response protocols are essential to prevent their establishment.
ANDREW F. VAN DEN HURK
Public Health Virology Forensic and Scientific Services, Department of Health, Queensland Government, PO Box 594, Archerfield, Qld 4108, Australia
[email protected]
Image: Figure 1. Andrew van den Hurk..