Bacterial sweepstake: big wins for infection control

Top view microorganisms Nutrient agar in plate. Credit: iStock/Sarawutnam
For over a century, the cornerstone of modern medicine has been a simple yet profound truth: cleanliness saves lives. Infection control is not merely a hospital policy; it is the fundamental shield that allows complex surgeries and life-saving treatments to occur safely. However, as we move further into the 21st century, we are discovering that this shield is being challenged by the very nature of the microbial world we inhabit.
We live in a world teeming with microscopic life. Bacteria are ubiquitous—many are essential to our health, while others exist benignly in the air we breathe and the surfaces we touch. Yet, in a hospital setting, this microbial diversity poses a unique paradox. In any space characterised by constant human activity, achieving a truly sterile environment is nearly impossible. This creates an ongoing challenge for healthcare facilities that house our most vulnerable populations. Patients in the intensive care unit (ICU) often lack the immune resilience of a healthy individual, meaning that otherwise harmless bacteria can become life-threatening opportunistic pathogens in a clinical ward.
The challenge is further complicated by the tools we use to fight back. While our modern arsenal of disinfectants and medicines eliminates the vast majority of problematic bacteria, it also inadvertently creates a "survival of the fittest" scenario. This is known as selective pressure. Bacteria reproduce through binary fission—a rapid process of exponential growth where one cell becomes two, then four, then eight. During this rapid division, random genetic mutations occur. Occasionally, a mutation grants a bacterium a "superpower," such as a molecular pump that flushes out antibiotics. When we apply cleaning chemicals, we kill the "weaker" bacteria but leave these mutated survivors to thrive and multiply. This is the primary driver of antimicrobial resistance (AMR), a silent crisis that renders our standard treatments ineffective.
To disrupt this cycle of resistance, we must move beyond broad-spectrum cleaning and toward precision monitoring. If we can identify exactly which bacteria are lurking in specific areas, we can target them with cleaning agents we know will be effective. Currently, most hospitals rely on traditional microbiology—taking a swab and trying to grow the bacteria in a lab. However, this method is limited; it usually only identifies specific, pre-determined species, and many bacteria simply refuse to grow in a lab setting. A newer alternative, metagenomics, sequences DNA directly from the environment. While highly detailed, metagenomics is prohibitively expensive and often fails because there is frequently too little raw DNA on a dry hospital surface to provide a complete picture.
This gap in our capabilities led to our core research question: Is there a middle ground? We hypothesised that a method called plate sweeps could provide the answer. In this approach, we take all the organisms that grow on a culture plate and sequence them collectively. This combines the affordability and focus of traditional culture with the high-resolution genetic data of sequencing, potentially offering a clearer view of hospital microbial diversity than ever before.
The perfect opportunity to test this theory arose at St Vincent’s Private Hospital Toowoomba in Queensland, Australia. Under the guidance of Dr. Jeremy Fernando, the ICU Director, the hospital was nearing the completion of a brand-new ICU wing in late 2023. This provided a rare "blank slate" for our research. We could sample the environment while it was still pristine and then track exactly how the microbial landscape changed once the doors opened to patients and staff.

This ambitious study was a collaborative effort bringing together experts from the University of Southern Queensland (UniSQ), Queensland University of Technology (QUT), St Vincent’s Hospital, and the University of Queensland. Led by myself and my Vacation Research Experience Student (VRES), Ms. Aasha McMurray-Jones, the team conducted intensive sampling throughout 2023 and 2024. They targeted every conceivable high-touch surface: doorknobs, desks, bed rails, light switches, and even the nooks and crannies of sinks and showers. These are the "highways" of bacterial transmission, where microbes hitch a ride from the environment to a patient.
After collection, the samples were transported to the QUT laboratories for overnight incubation. Any growth regardless of what it looked like was subjected to DNA extraction and sequencing. The results were a revelation. We found that the introduction of patients acted as a massive ecological "reset" for the ward. Before patients arrived, the ICU was occupied by "environmental" bacteria, microbes typically found in soil or water that rarely cause human illness. However, just two months after the ward opened, the microbial community had transformed completely. The environment became enriched with bacteria notorious for causing hospital-acquired infections. For instance, levels of Pseudomonas species—a leading cause of ventilator-associated pneumonia—tripled. Most alarmingly, even though we didn't specifically look for resistant strains, the genetic data showed that 93% of the bacteria found after patient introduction possessed some form of resistance. In contrast, 75% of the bacteria found in the empty ward had no resistance at all.

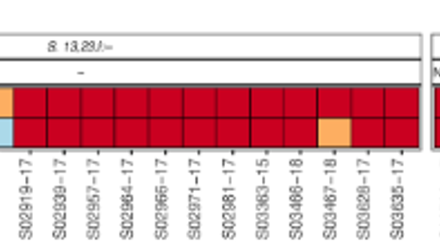
Beyond identifying what was there, our plate sweep method allowed us to track where the bacteria were going. By comparing DNA "fingerprints" across different locations, we identified 17 distinct sites that shared the exact same bacterial strains, proving that microbes were moving through the ward. The data pointed to a clear culprit for transmission: shared patient bathrooms. By identifying these specific hotspots, the hospital now has the actionable intelligence needed to implement targeted cleaning protocols, stopping the spread of dangerous bacteria before they reach a vulnerable patient.
So, were plate sweeps a success? This pilot study demonstrated that the method is a powerful tool for identifying resistance genes and mapping transmission pathways that traditional methods might miss. However, the journey is not over. While we have proven the value of the data, we have yet to perform a head-to-head comparison against traditional culture and metagenomics to determine the most cost-effective standard for hospitals worldwide. Our next step is a larger, multi-site comparative study to further refine this 'middle ground' method and ensure that our hospitals remain the safe havens of healing they were always meant to be.
Micro Scopes
Micro Scopes is an ongoing blog series by the Microbiology Society, written by microbiologists. This series brings you the latest and most exciting scientific findings published in the Society's journals and spotlights the perspectives of microbiologists around the world on their latest research.